Air-blown fiber solves today's healthcare IT needs

Characteristics that make the technology attractive in other venues also apply in healthcare settings.
By Clint Morgan, RCDD; National Electric Works
The surge of new and advanced communication and medical technologies: Voice over Internet Protocol (VoIP), emerging high-bandwidth imaging equipment, the convergence of clinical and information technology (IT) systems, and the migration toward electronic health records, is quickly transforming how healthcare is and will be delivered. Keeping pace with technology change, including new high-bandwidth security and energy-saving building automation systems is, however, only one of a multitude of challenges facing today's hospital and healthcare facilities. IT network and facilities managers also confront new and more stringent patient safety and infectious disease control restrictions, increasing federal and state regulatory changes, evolving environmental protocols for network sustainability, and plans for expansion despite filled conduit and duct bank problems, while being pressured to cut costs and to prove measurable return on investment.
To resolve all of these challenges, a growing number of major hospital and healthcare systems–including the National Institutes of Health (NIH), Mayo Clinic, Central DuPage Hospital, Kaiser Permanente, Penn State Milton S. Hershey Medical Center, and Sharp Healthcare– have adopted an end-to-end air-blown fiber (ABF) system in lieu of conventional optical fiber cabling systems.
Why? Unlike conventional fiber optic cabling systems that require the disruptive and time- and labor-intensive method used for decades of pulling optical fiber cable, the non-disruptive and environmentally clean air-blown fiber technology provides the healthcare facility with an immediately scalable, responsive, and sustainable LAN backbone. An ABF system allows the exact fiber types and counts to be blown in and out of the healthcare network when and where needed for fiber installations, upgrades and any moves, adds, and changes (MACs) in minutes or hours, thereby keeping up with critical network changes as they occur. That is, in real-time.

As demonstrated here, an air-blown fiber's tube-cable design provides a 322-percent increase in capacity within a conduit, compared to traditional cabled fiber.
Further defying the capabilities of traditional optical fiber cabling systems, air-blown fiber also eliminates the need and cost for infectious disease control preparatory processes, enabling fast and easy fiber installations and upgrades in minutes even in hard to reach and highly sanitized areas; invalidates the debate about whether to install OM3 or OM4 fiber; eliminates any disruption to the physical healthcare facility promoting patient safety; and resolves congested conduit and duct bank problems plaguing many of today's healthcare campuses. Advancing speed and efficiency, an air-blown fiber system reduces pathway costs and saves typically 70 to 90 percent of the time and costs for fiber-related projects associated with conventional cabling systems, yielding continuous return on investment that can significantly reduce the lifetime cost of ownership for the healthcare network.
By examining the components and methods of an air-blown fiber system, backed by actual case examples and cost data, design engineers, IT network and facilities managers can gain further insight about how air-blown fiber technology impacts their vision for the evolving, truly flexible, infectious disease controlled, 21st century hospital-healthcare LAN. Since air-blown fiber systems vary in capability, sustainability, speed, and performance, information provided in this article pertains to Sumitomo Electric Lightwaves's FutureFlex Air-blown Fiber System (www.futureflex.com). References to air-blown fiber or ABF in this article apply exclusively to the FutureFlex system.

Air-blown fiber bundles, like the FutureFlex bundles shown here, keep network administrators from having to estimate or guess the number of fibers they will need in five or six years' time.
Creating the real-time healthcare IT network
At the heart of the system is an infrastructure of tube cable, in a wide variety of outdoor and indoor riser and plenum rated options, that forms the healthcare campus' intrabuilding and in-building LAN topology, ultimately providing virtually unlimited fiber, bandwidth and pathway capacity. Unlike conventional cabling systems, the laying of the tube cable is the only occurrence of physical disruption to the healthcare facility and/or its grounds. The installation of the tube cable pathway eliminates pull points required every 100 to 200 feet required by conventional cabling systems, thereby reducing or eliminating labor-intensive work in manholes. The non-PVC tube cable contains up to 19 smaller empty tubes and can be either direct buried in the outside plant to replace both traditional conduit and innerduct for upfront infrastructure cost savings or is flexible enough to be placed in an existing conduit pathway.
To illustrate the extent of capacity provided by the tube cable, consider that a total of only 3, 1¼ -inch innerducts, through which conventional fiber optic cable is pulled, yield only 3 pathways in a standard 4-inch conduit. In that same 4-inch conduit, 2, 19- tube cables yield 38 pathways. Even if a popular fabric innerduct is used, which fits 9 conventional fiber optic cables that yield 9 pathways, the ABF tube cable still provides a 322 percent increase in capacity within the same space, resolving for the healthcare campus any congested conduit and duct bank problems and ensuring the likelihood of never having to lay additional conduit. Because of its virtually unlimited pathway space, the tube cable infrastructure needs to be installed only once. The same tube cable pathway, through which any fiber type and counts required can be quickly blown in and out, is reused time and time again, eliminating the need to re-enter the pathway or conduit system as is necessary with conventional cabling. A few spare tubes within the tube cable are always left empty for future expansion, truly futureproofing the healthcare network in real-time and eliminating the need and investment in dark fiber.
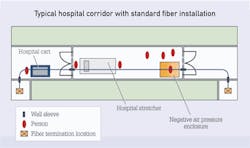
This diagram, provided by Chris Archer and Brian Zeiders of Brinjac Engineering, shows the congestion typical when a traditional cable install is taking place in an 8-foot hospital corridor.
The tube cables are joined in tube distribution units (TDUs) using easy push-fit connectors. TDUs, generally located in communication or telecom rooms, are used at tube cable pathway branching locations. Because the tube cables offer a modular solution and can be easily connected using the push-fit connectors, different pathway configurations, not easily or cost-effectively accomplished with conventional cabling, can be quickly devised. To reduce costs and improve efficiency, the tube cable pathway can be reconfigured to support multiple topologies, such as ring, hierarchical star and others simultaneously, integrating systems from HVAC, physical security, to communications under one common backbone. To further illustrate the versatility provided by the tube cable pathway and TDUs, consider that the healthcare campus is adding a building to the network, which would require a conventional cabling system to install conduit and innerduct from the new building to wherever the central data hub or communications room is housed. Then, a crew of installers must pull the fiber-optic cable that same distance. With this ABF system, tube cable needs to be extended only from the local or closest TDU to the new building with fiber blown back in minutes to the fiber termination unit in the central data hub, minimizing disruption and saving considerable dollars in installation time and pathway infrastructure costs.
Ready, set, blow
Due to the high cost and labor-intensive process of pulling fiber-optic cable for fiber installations and upgrades, traditional cabling systems force healthcare IT and facilities managers to predict or guess future changes in patient growth, departmental needs, data traffic, and emerging technology requirements for the next five to six years to determine which fiber types and counts to lay, adding dark or potentially unused fiber as insurance for uncertain future bandwidth requirements and MACs. In contrast, there is no uncertainty, no dark fiber, and no five- to six-year waits for major upgrades with an ABF system. The ABF system allows any type of fiber bundle and counts to be quickly and easily blown at speeds of up to 150 feet per minute using compressed air or nitrogen when and where needed in the healthcare network tube cable pathway in a smooth, continuous, splice-free fiber run that reduces attenuation and eliminates splicing points of potential network failure for a more reliable healthcare network. Air-blown fiber bundles use the same type of optical fibers as conventional cable with standard termination methods.

Use of an ABF system in a hospital avoids the use of a negative air pressure enclosure (NAPE) such as the one seen here.
Upgrades and any network moves, adds, and changes can now be accomplished quickly and easily, even in the most limited and sanitized areas of the hospital. Healthcare facility installers can literally blow out OM2 50-micron multimode fiber undamaged and blow in OS1 singlemode fiber between buildings 6,000 feet apart in a matter of hours without ever getting their hands dirty. The OM2 fiber can be reused in another part of the network preserving the initial fiber investment. The ability to blow in and out any fiber type and counts when and where needed creates a real-time, sustainable healthcare network with no end to the fiber lifecycle. Because the fiber installation is done behind the scenes in a communications room or data hub, using only two installers at each end of the run, there are no large work crews and no disruption to the healthcare facility buildings or grounds as is typical with conventional cabling systems.
Because exchanging fiber types as bandwidth requirements change is fast and easy with an air-blown fiber system, the current debate about whether to install OM3 50μm or OM4 50 μm is a non-issue. With the ABF system, the healthcare facility is always ready for a fast and inexpensive transition in a matter of minutes or hours.
Application examples, cost data
Sharp Healthcare of San Diego, named the number-one integrated healthcare network in California and 6th in the nation by SDI, has 8 hospital campuses and is a long-time and continuous user of the FutureFlex Air-blown Fiber System. The following two actual installation examples and cost data comparing the ABF installation to that of a conventional cabling system have been derived by National Electric Works (www.nationalelectricworks.com), the design and installation firm serving Sharp Heathcare for over a decade.
The examples assume both conventional and ABF underlying infrastructure pathways have been already installed.
Project summary: Connect the main distribution frame for Sharp Grossmont Hospital (located in new tower, basement level) to the women's center's intermediate distribution frame.
Details (page 22): 1,200 feet away through a difficult pathway; 12-strand singlemode fiber needed.
Project summary: Requires 12 strands of multimode fiber to be installed between two buildings in the Sharp Memorial Hospital Campus to improve fire-alarm system operation. Extensive duct bank system with maintenance holes runs throughout the campus. Maintenance holes are near a busy loading dock and in access areas to a hospital administration building.
Details (below): For a traditional fiber-optic installation, closing the dock for staff safety is an issue. For the ABF infrastructure it is not. ABF does not disrupt the campus because it requires no construction work. Installation of additional fiber for traditional infrastructure further crowds the conduit system, thereby limiting network capacity. Installation of a four-tube ABF system, and use of one of those tubes, allows for 300 percent growth.

Several different ABF tube systems are shown here. One option available as part of the FutureFlex system is a non-PVC tube that contains up to 19 smaller tubes and can be direct-buried in the outside plant or placed in an existing conduit pathway.
The examples are typical of the time and labor savings generated by the ABF system, which accelerates project completion time and accrues return on investment, resulting in decreased cost of ownership for the healthcare IT network.
Avoid ceiling-tile lifting
Unlike conventional cabling systems, ABF addresses one of the most important concerns of today's hospital-healthcare systems–that of infectious disease control and patient safety. Financial costs associated with hospital-acquired infections have risen to $27.5 billion in additional healthcare expenses annually, according to healthcare-informatics.com, while regulatory mandates for Medicare and Medicaid will no longer pay for hospital-acquired infections.
The most compelling value of the ABF system is that it eliminates disruptive construction work, re-entrance into conduit and ceilings, and any physical disruption to the hospital-healthcare campus buildings and grounds that can compromise infection control and safety for patients, staff, and visitors. Because fiber installations, upgrades, any network changes, and pathway reconfigurations are done in the confines of the communication or telecom room, ABF is immediately ICRA (Infection Control Risk Assessment) and Joint Commission compliant.
The clean and non-disruptive ABF system eliminates the time-consuming and costly infection control preparatory processes that conventional cabling must undergo when entering conduit, walls, and especially ceilings in order to accomplish fiber installations, upgrades and changes. Potentially toxic mold spores and airborne pathogens lie dormant above ceiling tiles or in walls until disturbed, posing direct threats to immune-deficient patients and to highly sanitized areas. Although conventional cabling systems use HEPA filtration units and NAPEs (negative air pressure enclosures) to help reduce the chances of infection, they cause other patient safety disruptions, such as moving patients, crowding hallways, and interrupting the critical work of healthcare staff.
The illustration on page 24, drawn to scale, represents a typical eight-foot-wide hospital corridor and shows how the NAPE, fiber-optic cable reel and contractors congest the corridor, making it difficult to push even a hospital stretcher through the area. Also, the installation of conventional cable through the wall sleeves requires the removal and replacement of firestopping material, which often demands that the NAPE be set up in front of corridor doors blocking access to treatment rooms, further disrupting staff workflow and the daily operations of the healthcare facility.
Air-blown fiber not only eliminates construction work and disruption; it also eliminates the time and cost of the infectious disease control procedures that often add 20 to 40 percent to the total project cost.
Healthcare is in the throes of a historic evolution, which requires a LAN backbone that simultaneously evolves with it. Air-blown fiber is the only system with the capabilities to do just that. Bill Spooner, senior vice president and chief information officer of Sharp Healthcare concludes, "With air-blown fiber we achieve strategic velocity, which is effecting change rapidly and effectively without interfering with our ongoing operations. FutureFlex also gives us the capacity and flexibility for future growth, protects us with patient safety requirements … and offers significant financial value."
Clint Morgan, RCDD, is vice president of National Electric Works (www.nationalelectricworks.com).
Past CIM Issues
Material & Labor ($70/hr) | Time | Conventional ($) | Air-Blown Fiber ($) |
1,200' 12 strand singlemode Plenum Fiber/ABF Fiber Bundles | $1,680 | $1,680 | |
1,200' plenum rated innerduct $.85/ft | $1,020 | -------- | |
Labor to set up infection control | 8 hrs | $ 560 | -------- |
Labor to install innerduct | 128 hrs | $8,960 | -------- |
Labor to couple tubes & test | 6 hrs | ------- | $420 |
Labor to pull conventional fiber optic cable vs. blowing fiber via ABF | 128 hrs vs. 4 hrs | $8,960 | $280 |
TOTAL COST | 400 Vs 10 Hrs. | $21,180 | $2,380 (89% Savings) |
Material & Labor ($75/hr) | Time | Conventional ($) | Air-Blown Fiber ($) |
1,200' 12 strand multimode Fiber/ABF fiber bundles + misc. materials | $2,160 fiber $1,000 misc. | $1,440 fiber bundle $500 | |
4 maint. hole prep and safety setup; pump manholes, verify air quality, pull strings etc | 24 hrs | $1,800 labor | ------- |
Install innerduct or fabric-type fiber protection through duct bank | 64 hrs | $1,100 material $4,800 labor | ------- |
Install plenum innerduct (underground conduit to above ceiling to route FACP) | 16 hrs | $180 material $1,200 labor | ------- |
Install new 4-tube tube cable ABF from TDUs to both sides of path to FACP | 20 hrs | ------ | $560 material $1,500 labor |
Couple tube in TDUs, verify pathway, pressure & obstruction testing | 3 hrs | ------- | $225 labor |
Labor to pull conventional fiber optic cable vs. blowing fiber via ABF | 64 hrs vs. 4 hrs | $4,800 | $300 |
TOTAL COST (assumes termination costs are equal) | 168 hrs vs. 27 hrs | $17,040 | $4,525 (73% Savings) |

